
STAR-PUs - should we still be using them?
- Authors:
-
Posted:
- Categories:

What are STAR-PUs?
Specific Therapeutic Group Age-Sex Related Prescribing Units (STAR-PUs) were first introduced back in 1995, in a paper by Lloyd et al.1 These units were created to help improve comparisons between prescribing at different GP practices, by accounting for differences in the age and sex groups registered with a practice. It is known that a patient’s age and sex can influence how likely they are to need a prescription for a medication in a particular therapeutic group, such as cardiovascular drugs, antidepressants, antibiotics, etc. STAR-PUs aim to account for this influence (more below). The most common use case for STAR-PUs (both in OpenPrescribing and more widely) is for antibiotic prescribing. This is largely driven by antimicrobial stewardship programs which have used comparisons of antibiotic prescribing to identify outliers in need of improvement. This blog will therefore largely focus on antibiotic STAR-PUs.
How are STAR-PUs calculated?
In the example of antibiotic prescribing, it is widely accepted that babies, young infants and the elderly are more susceptible to infection. Consequently, if a practice has a much higher proportion of very young or elderly patients they would be expected to issue more prescriptions for antibiotics. Similar can be said for females of normal working age when compared with males of the same age. STAR-PUs add higher weightings to groups where antibiotic prescribing is likely to be higher.
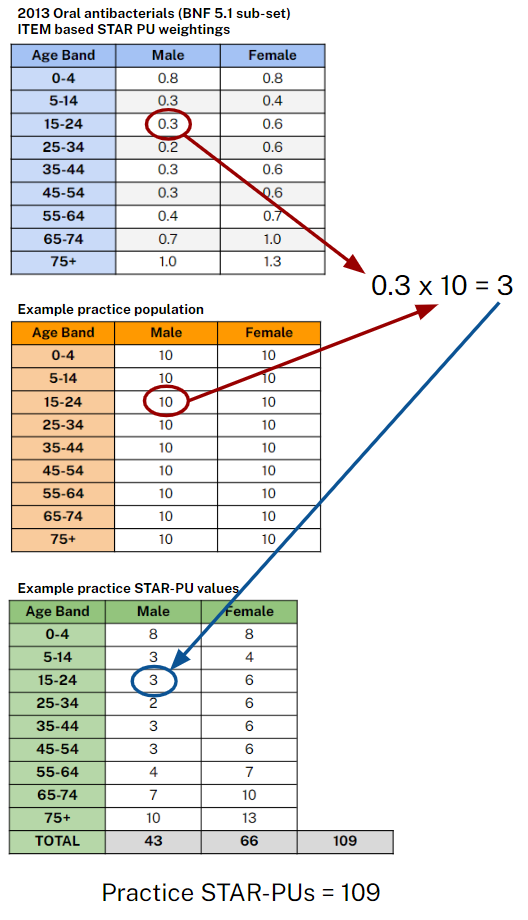
STAR-PU weightings for age-bands and sex have previously been published by NHS Digital with the last update in 2013. NHS Digital also publishes monthly data on patients registered at individual GP practices with breakdowns by specific age groups and sex. For each individual practice, the number of registered patients in each group is multiplied by the weighting and then each value is summed to give a STAR-PU value for the practice, see below for a worked example.
What’s the problem?
Although STAR-PUs make some attempts to account for age and sex variation between practice populations there are many other potential confounders which may affect prescribing. For example, for antibiotics, Pouwels et al. found that use of inhaled and systemic steroids are factors which would make an antibiotic prescription more likely,2 and Hope et al. found that prevalence of a number of comorbidities, smoking prevalence and deprivation were also linked to higher rates of antibiotic prescribing.3
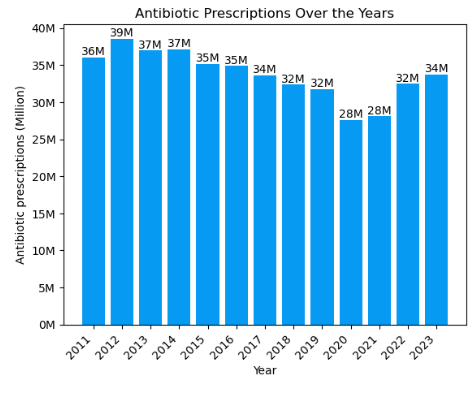
In addition to the above factors, prescribing can change with time and any weightings need to be updated to account for this. The last updates to STAR-PU weightings were made in 2013. Again using antibiotics as an example, there have been major changes over the last 11 years which have likely had a significant impact on how antibiotics are prescribed. These include changing guidelines, a move towards no antibiotics or back up antibiotic prescriptions for certain conditions, a rapid rise in remote and online consultation and of course, a global pandemic.
NHS Digital currently provides very limited information on their website regarding STAR-PUs and the current STAR-PU weightings being used can only be found via archived versions of the NHS Digital website. It therefore seems unlikely there is a plan to update the weightings in the near future.
What’s the alternative?
Currently the options are to either continue using 2013 STAR-PUs or revert to using list size. Use of potentially now outdated STAR-PUs adds an extra layer of complexity when trying to identify unwarranted variation, whereas moving back to list size re-introduces historic difficulties with comparison between practices.
Longer term, the increased availability of more granular patient data, for example via OpenSAFELY, presents opportunities for the development of new prescribing units encompassing a much wider range of factors not previously possible. This would, however, require time and investment.
What changes are planned to OpenPrescribing?
Currently we use item based STAR-PUs for oral antibiotics for the following measures on our site:
As STAR-PUs are only validated for oral antibiotics as a whole (not validated for subsets), we intend to change the co-amoxiclav, cephalosporins & quinolones prescribing volume measure to use list size (per 1000 registered patients) as the denominator. We have also recently launched a new fluoroquinolone measure which uses list size as the denominator.
We are also currently considering changing the volume of antibiotic prescribing measure to use list size as the denominator and removing the STAR-PU denominator option from the analyse page. But we want to hear your thoughts!
Before we make any changes to our STAR-PU measures we are keen to hear the thoughts from our users. If you have any thoughts, comments or suggestions on this topic or any part of OpenPrescribing please do not hesitate to get in touch with us, either by email or tagging us on X (formerly Twitter).
References
-
Lloyd DCEF , Harris CM, Roberts DJ. Specific therapeutic group age-sex related prescribing units (STAR-PUs): weightings for analysing general practices’ prescribing in England. BMJ 1995; 311: 991–4. https://doi.org/10.1136/bmj.311.7011.991 ↩︎
-
Koen B Pouwels, F Christiaan K Dolk, David R M Smith, Timo Smieszek, Julie V Robotham, Explaining variation in antibiotic prescribing between general practices in the UK, Journal of Antimicrobial Chemotherapy, Volume 73, Issue suppl_2, February 2018, Pages ii27–ii35, https://doi.org/10.1093/jac/dkx501 ↩︎
-
Hope, E. C., Crump, R. E., Hollingsworth, T. D., Smieszek, T., Robotham, J. V., & Pouwels, K. B. (2018). Identifying English Practices that Are High Antibiotic Prescribers Accounting for Comorbidities and Other Legitimate Medical Reasons for Variation. In EClinicalMedicine (Vol. 6, pp. 36–41). Elsevier BV. https://doi.org/10.1016/j.eclinm.2018.12.003 ↩︎